


ABSTRACT
Background: In January 2025, the British Columbia Centre for Disease Control (BCCDC) released an updated guideline with new breakpoints for ceftriaxone, cefixime, and azithromycin against Neisseria gonorrhoeae (N. gonorrhoeae). With increasing incidence of gonorrhoea cases in Canada, this study aimed to understand the antimicrobial susceptibility patterns of N. gonorrhoeae in British Columbia (BC) and examine the impact of different breakpoints.
Subin Mun1 and Eugene Y. H. Yeung, MD, MSc, BSc(Pharm), FRCPC, FCCM, D(ABMM), DTM&H, CTH, CIC, LTC-CIP1,2,3*
1 Faculty of Pharmaceutical Sciences, University of British Columbia, Vancouver, British Columbia, Canada
2 Faculty of Medicine, University of British Columbia, Vancouver, British Columbia, Canada
3 School of Medicine, Simon Fraser University, Surrey, British Columbia, Canada
*Corresponding author
Eugene Y.H. Yeung
LifeLabs
7455 130 St.
Surrey, BC V3W 1H8,
Canada
email: eugeney@doctors.org.uk
Article history:
Received 20 November 2025
Received in revised form 21 January 2026
Accepted 28 January 2026
ABSTRACT
Background: In January 2025, the British Columbia Centre for Disease Control (BCCDC) released an updated guideline with new breakpoints for ceftriaxone, cefixime, and azithromycin against Neisseria gonorrhoeae (N. gonorrhoeae). With increasing incidence of gonorrhoea cases in Canada, this study aimed to understand the antimicrobial susceptibility patterns of N. gonorrhoeae in British Columbia (BC) and examine the impact of different breakpoints.
Methods: The antimicrobial susceptibilities of 77 N. gonorrhoeae isolates from 2024, tested at LifeLabs BC, were analyzed using the Clinical and Laboratory Standards Institute (CLSI) and BCCDC breakpoints.
Results: The susceptibility rates of N. gonorrhoeae to ceftriaxone, cefixime, and azithromycin were 100%, 100%, and 87% with CLSI breakpoints, and 99%, 99%, and 70% with BCCDC breakpoints, respectively. The difference observed for azithromycin was statistically significant (p = 0.0107).
Conclusions: Ceftriaxone, a first-line treatment for gonorrhoea, remains favourable based on its activity data observed. However, the new BCCDC breakpoints may alter the annual azithromycin susceptibility rate, potentially causing an apparent increase in non-susceptibility. Close monitoring and annual reviews of N. gonorrhoeae cases may be warranted to provide valuable insights into evolving trends.
KEYWORDS:
Neisseria gonorrhoeae, ceftriaxone, azithromycin, antibiogram, pseudo-outbreak
INTRODUCTION
Neisseria gonorrhoeae (N. gonorrhoeae), also known as gonococcus (GC), is a Gram-negative diplococcus that colonizes the mucosal membranes, including genital, anorectal, oropharyngeal, and conjunctival regions, and causes gonorrhoea, a sexually transmitted infection (STI) (Centers for Disease Control and Prevention, 2022; Edwards & Apicella, 2004; Chan et al., 2016). In Canada, the number of gonorrhoea cases has been consistently increasing over the years, with a minor drop in 2020 during the COVID-19 pandemic (Government of Canada, 2023). However, the trend returned in 2021, with the incidence rising by 124% compared to 2012 (Government of Canada, 2023). Given the observed gonorrhoea cases, reduced susceptibility to previous empiric therapies (penicillin and tetracyclines), and the introduction of resistance to current empiric regimens (azithromycin, cefixime, and ceftriaxone), a comprehensive understanding and monitoring of the local resistance patterns is warranted (Government of Canada, 2024a, 2025; Sawatzky et al., 2025; Unemo & Shafer, 2014).
Nonetheless, the use of nucleic acid amplification tests (NAATs) with high sensitivity has changed the practice by reducing the need for culture and sensitivity testing. Currently, most diagnoses of gonorrhoea in Canada are confirmed with NAAT performed on first-void urine samples or vaginal, cervical, or urethral swabs (Government of Canada, 2024b). If positive, empiric therapy with ceftriaxone is given unless the case is considered complicated or the patient has an allergy or refuses an intramuscular route of treatment (Government of Canada, 2025). Although NAATs have accelerated care, they have also introduced a new gap. For example, because NAATs do not provide susceptibility data,
British Columbia (BC) lacks an updated antibiogram to guide local practitioners and confirm the adequacy of current practice. The most recent GC minimum inhibitory concentration (MIC) data for BC cover only the period from 2012 to 2021 (Wong et al., 2022).
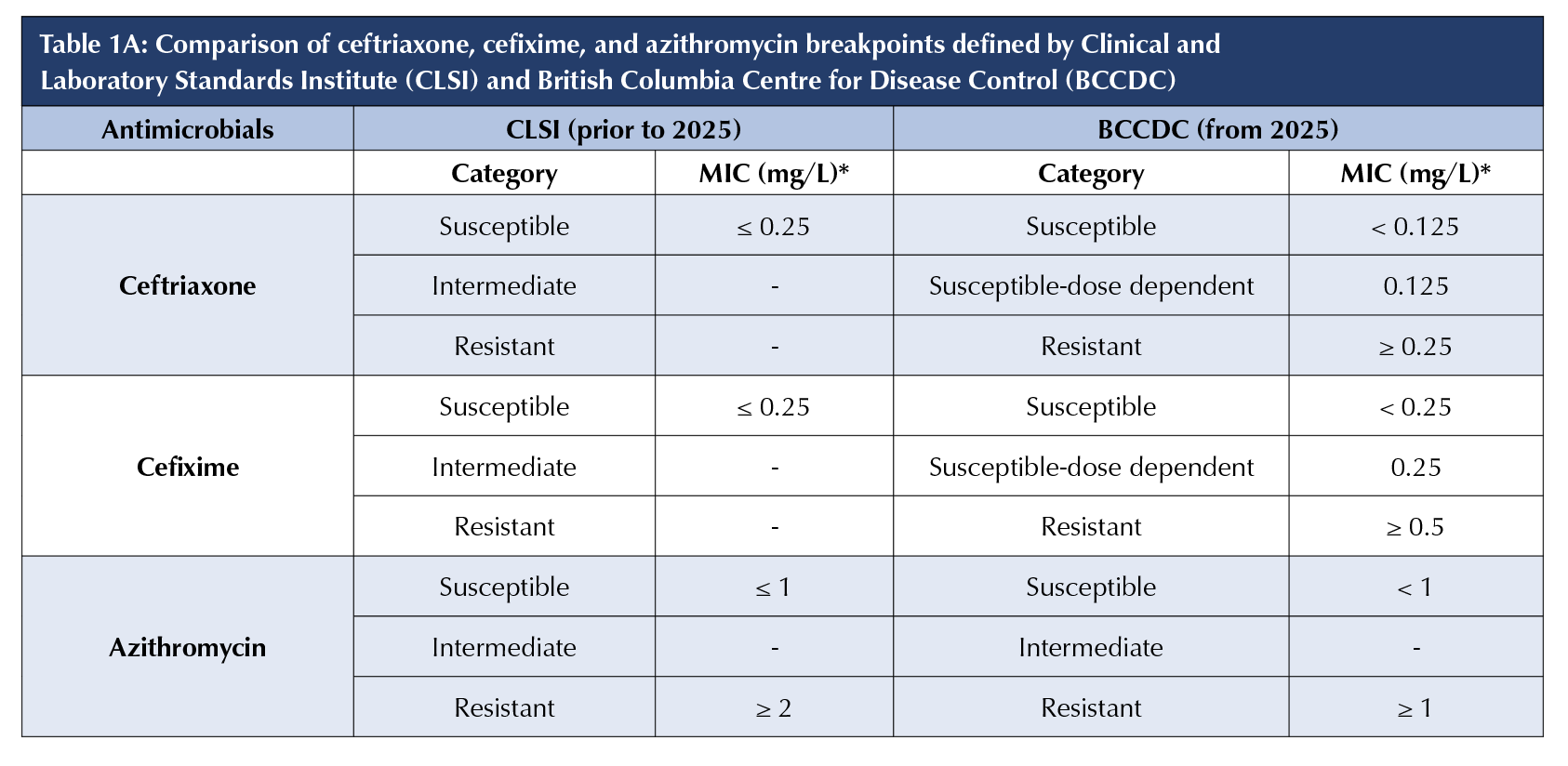
In January 2025, the BC Centre for Disease Control (BCCDC) released a new guideline with changes in breakpoints for third generation cephalosporins (ceftriaxone and cefixime) and azithromycin against GC (Table 1A) (Grant, 2025). Previous culture and sensitivity reports followed the Clinical and Laboratory Standards Institute (CLSI) M100 guideline, which does not provide resistance breakpoints for third-generation cephalosporins (Clinical and Laboratory Standards Institute, 2025). However, other international guidelines (e.g., European Committee on Antimicrobial Susceptibility Testing) have different breakpoints, defining resistance based on MIC values (European Committee on Antimicrobial Susceptibility Testing, 2025). Given these discrepancies, BCCDC’s newly adopted categories for third generation cephalosporins include “resistant”, identifying the ineffectiveness of an antibiotic, and “susceptible-dose dependent”, identifying organisms that require a greater drug exposure (Grant, 2025). In comparison, azithromycin’s MIC values for “susceptible” and “resistant” have been adjusted to distinguish between wild-type and resistant GC (Grant, 2025). No literature has yet reviewed the impact of the update on susceptibility data in BC.
Given these knowledge gaps, this study aimed to understand the characteristics of GC isolates in BC using susceptibility data obtained from GC isolates identified at LifeLabs BC. Additionally, with the adjustments to breakpoints, we examined the interpretation and significance by comparing the antibiogram created based on the previous CLSI guideline with the one created based on the new BCCDC guideline. Lastly, given the initiation of BC’s doxycycline post-exposure prophylaxis (PEP) program in December 2023 to prevent syphilis, chlamydia, and gonorrhoea, tetracycline susceptibility data have been analyzed to gauge the effectiveness of the initiative and provide a baseline to examine drug resistance development following frequent use of doxycycline (British Columbia Centre for Excellence, 2023).
METHODS
Data collection and analysis
Data for this retrospective study were gathered using the Microbiology Electronic Worksheet System (MEWS; Version 5.00.267; LifeLabs, Toronto, ON, Canada). The software organized data for all GC isolates identified at LifeLabs BC microbiology regional laboratories (Surrey and Victoria) between January 1 and December 31, 2024. To minimize any confounding variables, such as seasonal and practice differences, data from patients of all ages and genders over a one-year period were included. As recommended by CLSI, the minimum sample size for each antibiotic was set at 30 isolates (Clinical and Laboratory Standards Institute, 2025). The data were limited to community clinical specimens initially processed at one of the two LifeLabs BC microbiology regional laboratories, which included specimens from family medicine clinics, walk-in clinics, urgent care centres, and 129 LifeLabs patient service centres. Hospital inpatient specimens were not included in the current study. Moreover, this study did not include specimens from hospital sexual health clinics and long-term care centres with contracted laboratory service at their health authority regional microbiology laboratories.
GraphPad QuickCalcs (https://www.graphpad.com/quickcalcs/) was used for statistical analysis. Both two-tailed Fisher’s exact test and chi-square test were performed to compare categorical differences between groups. p < 0.05 was used when determining statistical significance.
Identification of microorganisms in culture
As per LifeLabs’ standardized procedures, GC isolates from the Lower Mainland were cultured at the Surrey regional microbiology laboratory, and GC isolates from Vancouver Island were cultured at the Victoria regional microbiology laboratory. Both laboratories operated using identical standard operating procedures in LifeLabs BC and are accredited by the College of Physicians and Surgeons of British Columbia Diagnostic Accreditation Program. All GC isolates were clinical isolates from patients and did not include surveillance samples.
When each specimen arrived at the designated regional microbiology laboratory, a chocolate agar plate and a Martin Lewis agar plate were inoculated and incubated at 35–37°C in CO2 for 72 hours. The first examination of both plates occurred after 18–24 hours of incubation, and ongoing daily monitoring continued for a total of 72 hours before the isolate was reported as negative. When colonies were not visible, they were rapidly returned to the incubator, thereby preventing viability loss from the absence of CO2. When suspicious colonies were noticed, an oxidase test was performed. When they were oxidase-positive, a Gram stain was performed to check for the presence of Gram-negative diplococci. Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) (Bruker Daltonics GmbH & Company KG, Bremen, Germany), followed by Aptima™ N. gonorrhoeae Assay (Hologic Incorporation, San Diego, CA, United States) or VITEK2 (bioMerieux Incorporated, Durham, N.C., United States) with Neisseria-Haemophilus identification card (NH), was performed on oxidase-positive suspicious colonies to confirm the identification of GC isolates. All GC isolates were stored frozen before being sent to BCCDC for antibiotic susceptibility testing (AST).
Antibiotic susceptibility testing
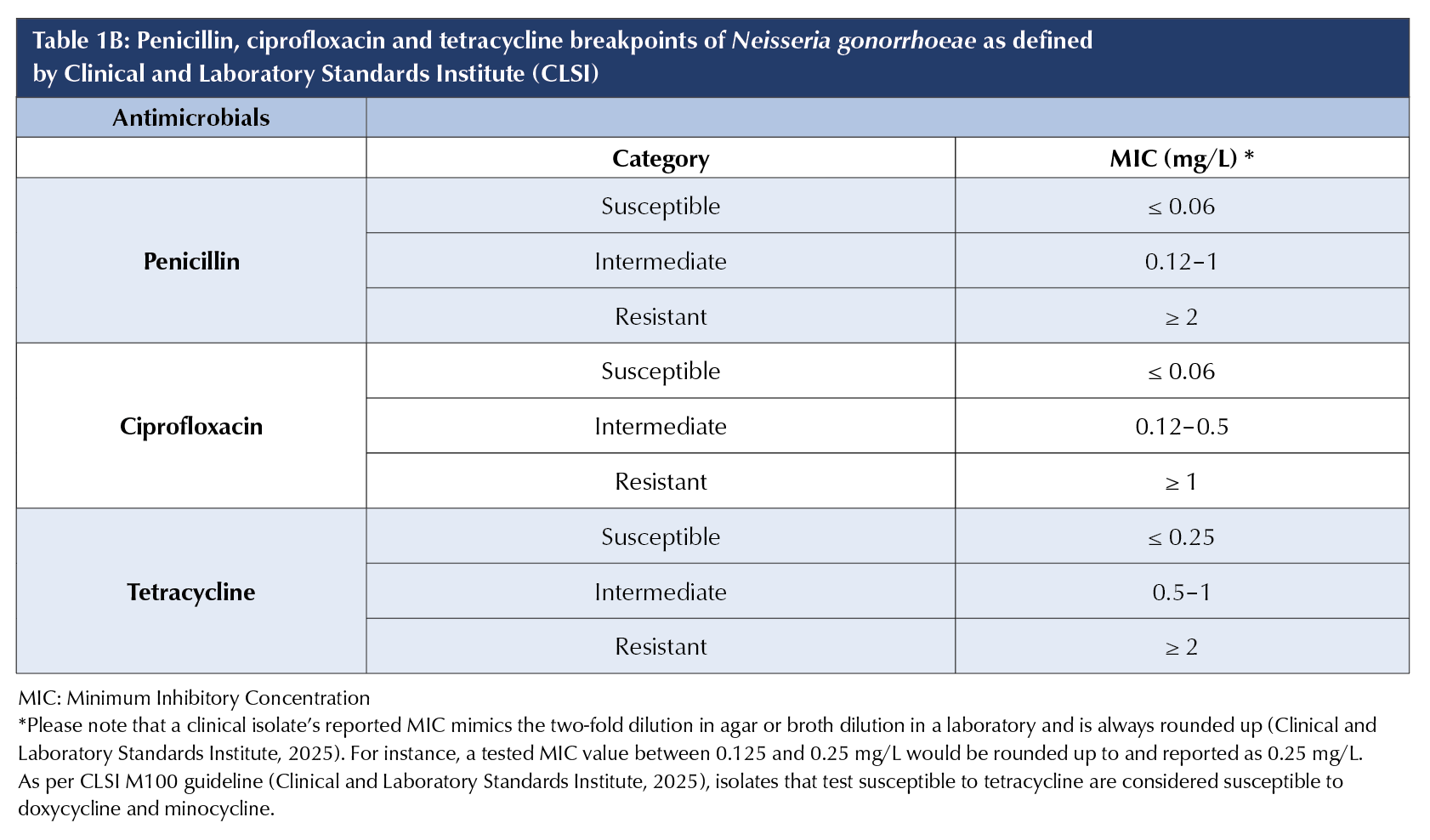
AST was performed on all cultured GC isolates using CLSI M100 standardized methods at the provincial laboratory (Clinical and Laboratory Standards Institute, 2025). The routine panel included penicillin, ciprofloxacin, tetracycline, azithromycin, cefixime, and ceftriaxone. The AST results were interpreted as susceptible, intermediate (applicable only to penicillin, ciprofloxacin, and tetracycline), or resistant, based on the breakpoints suggested in the CLSI M100 guideline (Table 1A and 1B). According to the same guideline, isolates that test susceptible to tetracycline are considered susceptible to doxycycline and minocycline. For this study, the MICs of azithromycin, cefixime, and ceftriaxone were reinterpreted using the new BCCDC breakpoints (Table 1A).
RESULTS
Identification of Neisseria gonorrhoeae isolates from different anatomical sites
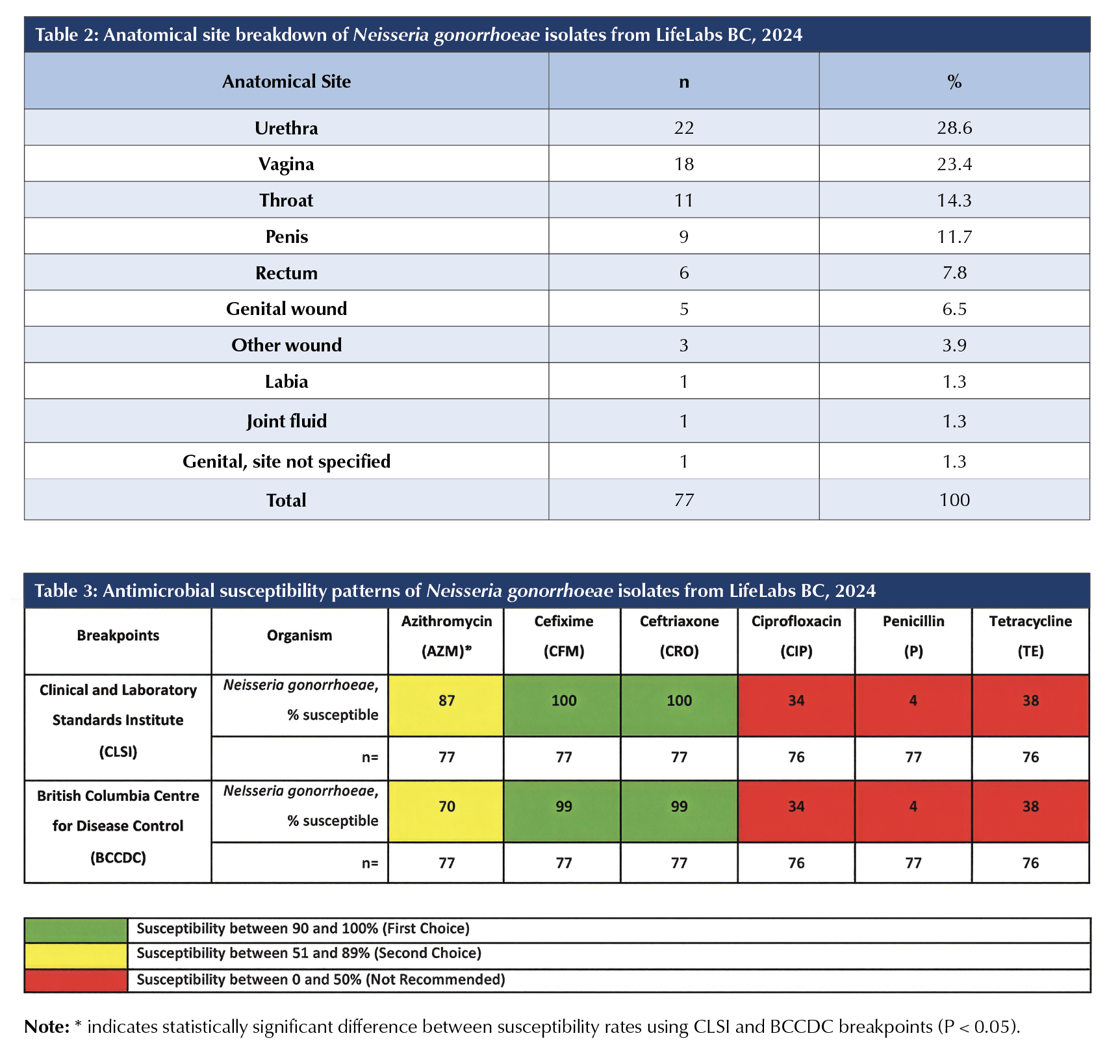
A total of 77 GC isolates were identified from January 1, 2024 through December 31, 2024, of which 57 originated from the Lower Mainland, with the rest from Vancouver Island. The mean age of the patients was 34.5 years (range: 16–64 years), and 25% were female (19/77). Table 2 lists the anatomical sites from which GC isolates were obtained.
Antimicrobial susceptibility profile of Neisseria gonorrhoeae isolates
The susceptibility patterns of 77 GC isolates are presented in Table 3. With the previous CLSI breakpoints, 87% of GC were susceptible to azithromycin, and 100% of GC were susceptible to both cefixime and ceftriaxone. With the new BCCDC breakpoints, 70% of GC were susceptible to azithromycin, and 99% of GC were susceptible to both cefixime and ceftriaxone.
The difference between susceptibility rates for azithromycin was found to be statistically significant with a p-value of 0.0107 using the chi-square test and 0.0176 using Fisher’s exact test. The difference between susceptibility rates for ceftriaxone was found to be not statistically significant with a p-value of 0.3157 using the chi-square test and 1.000 using Fisher’s exact test. GC showed the same susceptibility rates for cefixime and ceftriaxone, with no significant differences found. As the recent BCCDC update did not include ciprofloxacin, penicillin, or tetracycline, identical breakpoints were used for both antibiograms: 34%, 4%, and 38% of GC isolates were susceptible to ciprofloxacin, penicillin, and tetracycline, respectively.
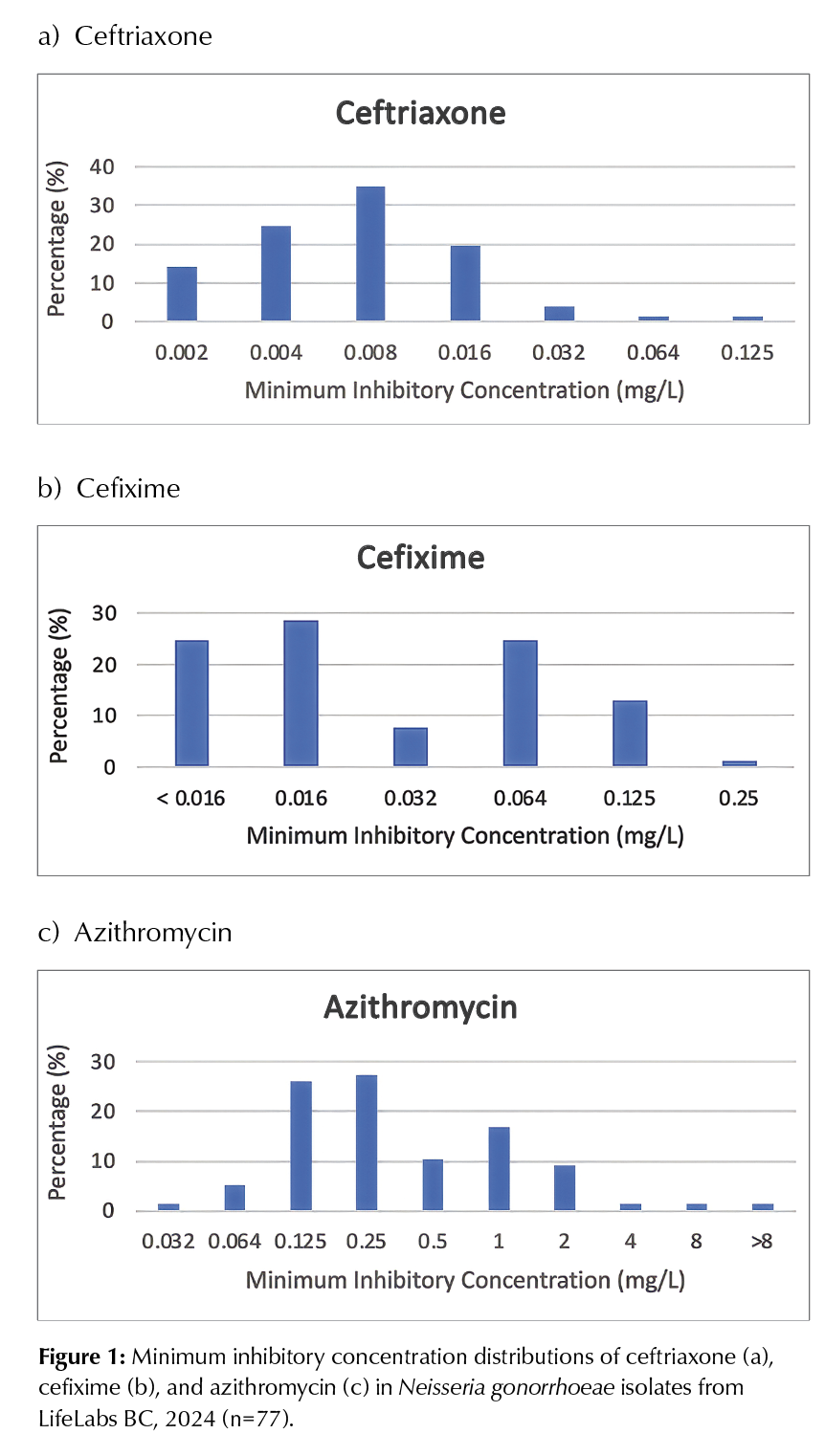
The MIC distributions of ceftriaxone, cefixime, and azithromycin in GC isolates are presented in Figures 1a-c. GC isolates had relatively low ceftriaxone MIC values (Figure 1a), with one isolate having a MIC of 0.125 mg/L, which is considered susceptible-dose dependent according to the new BCCDC guideline. One other isolate had a MIC of 0.064 mg/L, differing by no more than 1 log2 dilution from the new BCCDC breakpoint and demonstrating essential agreement (Humphries et al., 2018). A similar trend was observed for cefixime (Figure 1b), with one isolate having an MIC of 0.25 mg/L, which is considered susceptible-dose dependent according to the new BCCDC guideline. However, 10 isolates (13%) had an MIC of 0.125 mg/L, showing essential agreement with the new BCCDC breakpoint. For azithromycin (Figure 1c), 13 isolates (17%) had an MIC of 1 mg/L, which is considered resistant according to the new BCCDC guideline, and eight isolates had an MIC of 0.5 mg/L, showing essential agreement with the BCCDC breakpoint.
DISCUSSION
Current empiric treatment for Neisseria gonorrhoeae (implications for clinicians)
In recent years, a fluctuation in antibiotic susceptibility of GC to cefixime, ceftriaxone, and azithromycin across Canada has raised concerns (Government of Canada, 2025; Sawatzky et al., 2025). With azithromycin resistance surpassing 5% in 2016, the empiric choice for uncomplicated gonorrhoea for adults and adolescents 10 years of age or older became ceftriaxone 500 mg by intramuscular (IM) injection as a single dose (Government of Canada, 2025). The CLSI breakpoint for ceftriaxone used until recently in BC is based on an intravenous (IV) regimen of ceftriaxone 1g every 24 hours (Clinical and Laboratory Standards Institute, 2025). However, studies showing the similarity of ceftriaxone’s IM and IV pharmacokinetics and plasma concentrations following a 500 mg IM dose and a 1g IV dose have made the use of an IM injection with the lowest possible dose a viable option (Goonetilleke et al., 1996; Scully et al., 1984). A recent study by St. Cyr et al. further supports this dosing, suggesting that a 500 mg dose provides the needed antibiotic concentration for over 20–24 hours, which is a requirement for GC eradication based on Monte Carlo modelling (St. Cyr et al., 2020). Given the high susceptibility of GC to third-generation cephalosporins and stricter breakpoints in BC, ceftriaxone 500 mg IM as a single dose is a reasonable choice for empirical therapy. When ceftriaxone is not a feasible option, alternative regimens, such as cefixime 800 mg PO as a single dose plus azithromycin 1g PO as a single dose or cefixime 800 mg PO as a single dose plus doxycycline 100 mg PO twice daily for 7 days, can be used (Government of Canada, 2025).
Changes in breakpoints (implications for epidemiologists, laboratorians, and infection preventionists)
MIC interpretations change periodically, depending on how microorganisms evolve and regional practices change (Kowalska-Krochmal & Dudek-Wicher, 2021). Specifically, changes in breakpoints can occur when patients infected with an identical organism with a broad range of MICs do not show a significant difference in response after taking the same regimen of medication (Parry et al., 2015). A summary of clinical trials exploring azithromycin against Salmonella enterica serovar Typhi and serovar Paratyphi A with varying MICs serves as an example (Parry et al., 2015). Alternatively, changes in breakpoints could suggest a change in local practices, resulting in the categorization of microorganisms presenting with low levels of resistance, which could be eradicated with a greater drug exposure (Kowalska-Krochmal & Dudek-Wicher, 2021).
A considerable concern with changes in breakpoints is the potential for misinterpretation, particularly in the context of an outbreak of a resistant strain. This confusion could occur when susceptibility rapidly drops with the new breakpoint value, but a significant portion of the strains would not be considered resistant under the previous guideline. This case is supported by the two susceptibility reports for azithromycin generated using different guidelines (CLSI and BCCDC). Based on the 77 isolates analyzed, 13 isolates had an MIC of 1mg/L, a value now indicative of a resistant strain. The susceptibility of GC to azithromycin dropped from 87% to 70%, which is a statistically significant difference (p-value of 0.0107 using the chi-square test and p = 0.0176 using Fisher’s exact test). Nonetheless, this increase in resistance does not necessarily indicate an outbreak of a resistant strains; rather it is likely due to the change in the interpretation. The current data does not necessarily advocate for or against the changes in MIC breakpoints as evidence to support either side is still lacking. Rather, our data suggests close monitoring and annual reviews of N. gonorrhoeae cases to provide valuable insights into evolving trends. Our findings raise awareness of the potential for a pseudo-outbreak due to changes in breakpoints.
To the best of our knowledge, this paper presents the most up-to-date enhanced anti-biogram for GC, highlighting regional susceptibility patterns in BC. Since the current practice favours NAAT for the laboratory diagnosis of GC, this paper may serve as a valuable guide, setting the baseline for monitoring local trends. Moreover, additional analyses in the current study showed that the change in MIC interpretations would not alter GC’s susceptibility data for the first-line treatment, ceftriaxone. However, given that the azithromycin and cefixime combination is used as a second-line treatment, it is worth noting that the change in susceptibility data implies neither a decrease in the effectiveness of azithromycin nor an outbreak of azithromycin-resistant GC strains.
Clinical considerations for doxycycline post exposure prophylaxis
The DoxyPEP trial, which took place in San Francisco and Seattle in the United States, demonstrated the preventative benefit of doxycycline prophylaxis against STIs among men who have sex with men (MSM) and transgender women (Luetkemeyer
et al., 2023). A dose of doxycycline taken within 72 hours after condomless sex reduced gonorrhoea infection by approximately 55% with the regional baseline tetracycline resistance rate of 27% (Luetkemeyer et al., 2023). However, the tetracycline resistance rate is much lower than what we observed in British Columbia (62%). Given the different baseline resistance patterns, the possibility of observing suboptimal effectiveness of doxycycline PEP against GC should be considered. A meta-analysis examining the efficacy of doxycycline PEP revealed a 45% decrease in the risk of gonorrhoea with a range of effectiveness across the included studies, further supporting the concept that the clinical benefit of this prophylaxis can vary depending on the local resistance pattern (Leung et al., 2025). Additionally, as no studies have examined the impact of doxycycline PEP on changes in GC resistance patterns yet, therefore, no assumptions can be made about the consequences of increased doxycycline use. As tetracycline resistance is rare in Chlamydia trachomatis and Treponema pallidum, the development of drug-resistant strains is much less of a concern (Tien et al., 2020; Sanchez et al., 2020; Tantalo et al., 2025).
The emergence of drug-resistant strains of other pathogens should also be considered. According to a systematic review reporting the resistance pattern in normal human flora, exposure to oral tetracyclines for two to 18 weeks increased resistance in subgingival, gastrointestinal, and upper respiratory tract flora (Truong et al., 2022). Furthermore, a recent study examining participants from the DoxyPEP trial demonstrated that the use of doxycycline PEP increased the presence and expression of tetracycline resistance genes in the gut after six months, despite no change in the overall diversity of gut bacteria (Chu et al., 2025). Given that more frequent exposure to doxycycline increases the number of tetracycline resistance genes, closer monitoring of the development of doxycycline-resistant pathogens is crucial, given the widespread use of doxycycline to treat various acute conditions (Chu et al., 2025).
Comparison to other studies
A summary of GC’s MIC data of BC from 2012 to 2021 revealed that GC isolates with MIC values indicative of susceptible-dose dependent or resistant were observed in 17 out of 4,703 cases (0.4%) and 9 out of 4,703 cases (0.2%) with cefixime and ceftriaxone, respectively (Wong et al., 2022). When the 2012- 2021 data were compared with the 2024 data, the prevalence of susceptible-dose dependent or resistant isolates for cefixime (0.4% and 1.3%, respectively) and ceftriaxone (0.2% and 1.3%, respectively) was similar.
In contrast, the difference was evident for azithromycin. When MIC ≥ 2 mg/L (the previous CLSI breakpoint) was used to compare the prevalence of resistant strains due to data unavailability with the new BCCDC breakpoint (MIC ≥ 1 mg/L), the resistance rate was 1.7% (82/4703) from 2012 to 2021, compared with 13% in 2024 (Wong et al., 2022). Even though a direct comparison is needed to draw a definitive conclusion, the difference was approximately 11.3%, suggesting an increase in azithromycin-resistant strains compared with previous years.
Comparing against the ceftriaxone’s MIC data available from 21 European Union and European Economic Area (EU/EEA) countries in 2013, the BC MIC data look promising. Among 1,932 isolates from 21 other EU/EEA countries, the proportions with MICs of 0.002 mg/L, 0.004 mg/L, 0.008 mg/L, 0.016 mg/L, and 0.032 mg/L were approximately 15-18% each, whereas the proportions with MICs of 0.064 mg/L and 0.125 mg/L were around 14% and 3%, respectively (The Euro-GASP Network et al., 2015). Comparing the current BC data with EU/EEA data (Figure 1a), a greater percentage of GC isolates in BC had lower MIC values, suggesting the reduced susceptibility is less of a concern.
Study strengths and limitations
This study presents data solely from community settings, providing an updated antibiogram for community-reported GC. However, as a hospital dataset was not included, the current study should not be generalized to different clinical contexts. Additionally, we provided BC-specific data, demonstrating a regional susceptibility that can be used to monitor future changes. Nevertheless, the primary limitation of a localized antibiogram is that data must be extrapolated with caution to other jurisdictions in Canada and beyond. Given the variation in practices and resistance patterns across provinces and territories, developing localized antibiograms may offer clinical benefits. Continuous monitoring of GC cases along with annual antibiogram updates in BC might lead to faster recognition of resistant GC strain outbreaks. Furthermore, given that has begun, the effectiveness of the doxycycline PEP initiative and emerging resistance patterns should be explored.
CONCLUSIONS
This one-year study confirmed that ceftriaxone 500mg IM as a single dose is likely a suitable empiric treatment for uncomplicated gonorrhoea cases in BC However, considering the presence of GC strains resistant to azithromycin and the potential for problematic misinterpretation of susceptibility data due to breakpoint changes, closer monitoring of GC cases is warranted. Therefore, conducting continuous annual reviews of GC cases may provide valuable insights by enabling vigilant monitoring of evolving trends in the community. Additional studies are needed to evaluate the effectiveness of doxycycline PEP and its impact on GC resistance patterns.
REFERENCES
British Columbia Centre for Excellence. (2023, December). Doxycycline for bacterial sexually transmitted infection
(B-STI) prevention.
https://bccfe.ca/doxycycline-for-bacterial-sexually-transmitted-infection-b-sti-prevention/
Centers for Disease Control and Prevention. (2022, September 21). Gonococcal infections among adolescents and adults.
https://www.cdc.gov/std/treatment-guidelines/
gonorrhea-adults.htm
Chan, P. A., Robinette, A., Montgomery, M., Almonte, A., Cu-Uvin, S., Lonks, J. R., Chapin, K. C., Kojic, E. M., & Hardy, E. J. (2016). Extragenital infections caused by Chlamydia trachomatis and Neisseria gonorrhoeae: A review of the literature. Infectious Diseases in Obstetrics and Gynecology, 2016, 5758387. https://doi.org/10.1155/2016/5758387
Chu, V. T., Glascock, A., Donnell, D., Grabow, C., Brown, C. E., Ward, R., Love, C., Kalantar, K. L., Cohen, S. E., Cannon, C., Woodworth, M. H., Kelley, C. F., Celum, C., Luetkemeyer,
A. F., & Langelier, C. R. (2025). Impact of doxycycline
post-exposure prophylaxis for sexually transmitted infections on the gut microbiome and antimicrobial resistome.
Nature Medicine, 31(1), 207–217.
https://doi.org/10.1038/s41591-024-03274-2
Clinical and Laboratory Standards Institute. (2025). Performance standards for antimicrobial susceptibility testing (35th ed.).
Clinical and Laboratory Standards Institute (Eds.). (2022). Analysis and presentation of cumulative antimicrobial susceptibility test data (5th ed.).
Edwards, J. L., & Apicella, M. A. (2004). The molecular mechanisms used by Neisseria gonorrhoeae to initiate infection differ between men and women. Clinical Microbiology Reviews, 17(4), 965–981.
https://doi.org/10.1128/CMR.17.4.965-981.2004
European Committee on Antimicrobial Susceptibility Testing. (2025). Clinical breakpoints—Breakpoints and guidance.
https://www.eucast.org/clinical_breakpoints
Goonetilleke, A. K. E., Dev, D., Aziz, I., Hughes, C., Smith, M. J., & Basran, G. S. (1996). A comparative analysis of pharmacokinetics of ceftriaxone in serum and pleural fluid in humans: A study of once daily administration by intramuscular and intravenous routes. Journal of Antimicrobial Chemotherapy, 38(6), 969–976.
https://doi.org/10.1093/jac/38.6.969
Government of Canada. (2023, October). Chlamydia,
gonorrhea and infectious syphilis in Canada: 2021
surveillance data update.
https://www.canada.ca/en/public-health/services/publications/diseases-conditions/chlamydia-gonorrhea-infectious-syphilis-2021-surveillance-data.html
Government of Canada. (2024a, December 23). Gonorrhea guide: Etiology and epidemiology.
https://www.canada.ca/en/public-health/services/
infectious-diseases/sexual-health-sexually-transmitted-
infections/canadian-guidelines/gonorrhea/etiology-epidemiology.html
Government of Canada. (2024b, December 23). Gonorrhea guide: Key information and resources.
https://www.canada.ca/en/public-health/services/infectious-diseases/sexual-health-sexually-transmitted-infections/canadian-guidelines/gonorrhea.html
Government of Canada. (2025, May 14). Gonorrhea guide: Treatment and follow-up.
https://www.canada.ca/en/public-health/services/infectious-diseases/sexual-health-sexually-transmitted-infections/canadian-guidelines/gonorrhea/treatment-follow-up.html
Grant, J. M. (2025, January 31). Changes in reporting and interpretation of Neisseria gonorrhoeae susceptibility tests.
BC Centre for Disease Control.
http://www.bccdc.ca/resource-gallery/Documents/Guidelines%20and%20Forms/Forms/Labs/BCCDC%20PHL%20Memo_Changes%20in%20reporting%20and%20interpretation%20of%20N.%20gonorrhoea%20susceptibility%20tests.pdf
Humphries, R. M., Ambler, J., Mitchell, S. L., Castanheira, M.,
Dingle, T., Hindler, J. A., Koeth, L., Sei, K., Hardy, D.,
Zimmer, B., Butler-Wu, S., Dien Bard, J., Brasso, B., & Shawar, R. (2018). CLSI Methods Development and Standardization Working Group best practices for evaluation of antimicrobial susceptibility tests. Journal of Clinical Microbiology, 56(4), e01934-17. https://doi.org/10.1128/JCM.01934-17
Kowalska-Krochmal, B., & Dudek-Wicher, R. (2021). The
minimum inhibitory concentration of antibiotics: Methods, interpretation, clinical relevance. Pathogens, 10(2), 165.
https://doi.org/10.3390/pathogens10020165
Leung, V., Toy, J., Phillips, P., & Montaner, J. S. G. (2025). Doxycycline postexposure prophylaxis to prevent bacterial sexually transmitted infections. Canadian Medical Association Journal, 197(19), E534–E535.
https://doi.org/10.1503/cmaj.250128
Luetkemeyer, A. F., Donnell, D., Dombrowski, J. C., Cohen, S., Grabow, C., Brown, C. E., Malinski, C., Perkins, R., Nasser, M., Lopez, C., Vittinghoff, E., Buchbinder, S. P., Scott, H., Charlebois, E. D., Havlir, D. V., Soge, O. O., & Celum, C. (2023). Postexposure doxycycline to prevent bacterial sexually transmitted infections. New England Journal of Medicine, 388(14), 1296–1306.
https://doi.org/10.1056/NEJMoa2211934
Parry, C. M., Thieu, N. T. V., Dolecek, C., Karkey, A.,
Gupta, R., Turner, P., Dance, D., Maude, R. R., Ha, V.,
Tran, C. N., Thi, P. L., Be, B. P. V., Phi, L. T. T., Ngoc, R. N., Ghose, A., Dongol, S., Campbell, J. I., Thanh, D. P.,
Thanh, T. H., … Baker, S. (2015). Clinically and microbiologically derived azithromycin susceptibility breakpoints for Salmonella enterica serovars Typhi and
Paratyphi A. Antimicrobial Agents and Chemotherapy,
59(5), 2756–2764. https://doi.org/10.1128/AAC.04729-14
Sanchez, A., Mayslich, C., Malet, I., Grange, P., Janier, M.,
Saule, J., Martinet, P., Robert, J., Moulene, D., Truchetet, F., Pinault, A., Vermersch-Langlin, A., Benhaddou, N., Chanal, J., & Dupin, N. (2020). Surveillance of antibiotic resistance genes in Treponema pallidum subspecies pallidum from patients
with early syphilis in France. Acta Dermato-Venereologica, 100(14), adv00221.
https://doi.org/10.2340/00015555-3589
Sawatzky, P., Thorington, R., Barairo, N., Lefebvre, B., Diggle, M., Hoang, L., Patel, S., Van Caessele, P., Minion, J.,
Desnoyers, G., Haldane, D., Ding, X., Lourenco, L., Gravel, G., & Martin, I. (2025). Antimicrobial susceptibilities of Neisseria gonorrhoeae in Canada, 2022. Canada Communicable Disease Report, 51(4), 129–136.
https://doi.org/10.14745/ccdr.v51i04a03
Scully, B. E., Fu, K. P., & Neu, H. C. (1984). Pharmacokinetics of ceftriaxone after intravenous infusion and intramuscular injection. The American Journal of Medicine,
77(4C), 112–116.
St. Cyr, S., Barbee, L., Workowski, K. A., Bachmann, L. H., Pham, C., Schlanger, K., Torrone, E., Weinstock, H., Kersh, E. N.,
& Thorpe, P. (2020). Update to CDC’s treatment guidelines for gonococcal infection, 2020. MMWR. Morbidity and Mortality Weekly Report, 69(50), 1911–1916.
https://doi.org/10.15585/mmwr.mm6950a6
Tantalo, L. C., Luetkemeyer, A. F., Lieberman, N. A. P., Nunley, B. E., Avendaño, C., Greninger, A. L., Celum, C., & Giacani, L. (2025). In vitro exposure of Treponema pallidum to subbactericidal doxycycline did not induce resistance: Implications for doxycycline postexposure prophylaxis. The Journal of Infectious Diseases, 231(3), 729–733.
https://doi.org/10.1093/infdis/jiae381
The Euro-GASP Network, Cole, M. J., Spiteri, G., Jacobsson, S., Pitt, R., Grigorjev, V., & Unemo, M. (2015). Is the tide turning again for cephalosporin resistance in Neisseria gonorrhoeae in Europe? Results from the 2013 European surveillance. BMC Infectious Diseases, 15, 321.
https://doi.org/10.1186/s12879-015-1013-x
Tien, V., Punjabi, C., & Holubar, M. K. (2020).
Antimicrobial resistance in sexually transmitted infections. Journal of Travel Medicine, 27(1), taz101.
https://doi.org/10.1093/jtm/taz101
Truong, R., Tang, V., Grennan, T., & Tan, D. H. S. (2022). A systematic review of the impacts of oral tetracycline class antibiotics on antimicrobial resistance in normal human flora. JAC–Antimicrobial Resistance, 4(1), dlac009.
https://doi.org/10.1093/jacamr/dlac009
Unemo, M., & Shafer, W. M. (2014). Antimicrobial resistance in Neisseria gonorrhoeae in the 21st century: Past, evolution, and future. Clinical Microbiology Reviews, 27(3), 587–613.
https://doi.org/10.1128/CMR.00010-14
Wong, J., Chang, Y., Sorge, J., Ryan, V., Grennan, T., & Hoang, L. (2022, August). Antimicrobial resistant gonorrhea in BC, 2012–2021. BC Centre for Disease Control.
http://www.bccdc.ca/resource-gallery/Documents/Statistics%20and%20Research/Statistics%20and%20Reports/STI/STI_Annual_Report_2021_AMR_GC_
FINAL.pdf
Competing interests: Subin Mun has no competing interests to declare. Eugene Y.H. Yeung has been paid to work as a physician, pharmacist, microbiologist, and clinical assistant professor. Opinions expressed are solely his own and do not represent the views of his employers.
Acknowledgements: The authors would like to thank Dr. Marion Pearson, Professor at the Faculty of Pharmaceutical Sciences, University of British Columbia, for her support in this project. In addition, we would like to thank all the LifeLabs microbiologists and medical laboratory assistants and technologists, and information technology personnel for their technical support in the study.