Reprinted with permission from University of Toronto Press (https://utpjournals.press), DOI: 10.3138/jammi-2021-0012;
Official Journal of the Association of Medical Microbiology and Infectious Disease Canada.
Alice Zhabokritsky MD, MSc1, Nick Daneman MD, MSc1,2, Scott MacPhee MN-NP3, Jose Estrada-Codecido MSc4,
Aimee Santoro MSc, PHCNP5, Adrienne Kit Chan MD, MPH1,2, Philip Wai-Hei Lam MD, MSc1,2, Andrew Simor MD1,2,
Jerome Allen Leis MD, MSc1,2, Samira Mubareka MD1,2, Nisha Andany MD, MPH1,2
1Department of Medicine, University of Toronto, Toronto, Ontario, Canada
2Division of Infectious Diseases, Sunnybrook Health Sciences Centre, University of Toronto, Toronto, Ontario, Canada
3Department of Nursing, Sunnybrook Health Sciences Centre, University of Toronto, Toronto, Ontario, Canada
4Sunnybrook Research Institute, Sunnybrook Health Sciences Centre, University of Toronto, Toronto, Ontario, Canada
5Department of Obstetrics and Gynecology, Sunnybrook Health Sciences Centre, University of Toronto, Toronto, Ontario, Canada
Corresponding author:
Nisha Andany, MD, MPH
Sunnybrook Health Sciences Centre
2075 Bayview Avenue,
Room H2 66
Toronto, Ontario M4N 3M5
Canada
Tel: 416-480-6100 ext. 6044
Fax: 416-480-4786
E-mail: nisha.andany@sunnybrook.ca
ABSTRACT
Background: Most individuals with coronavirus disease 2019 (COVID-19) experience mild symptoms and are managed in the outpatient setting. The aim of this study was to determine whether self-reported symptoms at the time of diagnosis can identify patients at risk of clinical deterioration.
Methods: This was a retrospective cohort study of 671 outpatients with laboratory-confirmed COVID-19 diagnosed in Toronto between March 1 and October 16, 2020. We examined the association between patients’ baseline characteristics and self-reported symptoms at the time of diagnosis and the risk of subsequent hospitalization.
Results: Of 671 participants, 26 (3.9%) required hospitalization. Individuals aged 65 years or older were more likely to require hospitalization (odds ratio [OR] 5.29, 95% CI 2.19 to 12.77), whereas those without medical comorbidities were unlikely to be hospitalized (OR 0.02, 95% CI 0.00 to 0.17). After adjusting for age and presence of comorbidities, sputum production (adjusted OR [aOR] 5.01, 95% CI 1.97 to 12.75), arthralgias (aOR 4.82, 95% CI 1.85 to 12.53), diarrhea (aOR 4.56, 95% CI 1.82 to 11.42), fever (aOR 3.64, 95% CI 1.50 to 8.82), chills (aOR 3.62, 95% CI 1.54 to 8.50), and fatigue (aOR 2.59, 95% CI 1.04 to 6.47) were associated with subsequent hospitalization.
Conclusions: Early assessment of symptoms among outpatients with COVID-19 can help identify individuals at risk of clinical deterioration. Additional studies are needed to determine whether more intense follow-up and early intervention among high-risk individuals can alter the clinical trajectory of and outcomes among outpatients with COVID-19.
KEYWORDS
COVID-19, hospitalization, outpatients, symptoms
ABSTRAT
Historique : La plupart des personnes atteintes de la maladie à coronavirus 2019 (COVID-19) éprouvent des symptômes légers et sont prises en charge en milieu ambulatoire. La présente étude visait à déterminer si les symptômes autodéclarés au moment du diagnostic permettent de dépister les patients à risque de
détérioration clinique.
Méthodologie : Les chercheurs ont réalisé la présente étude de cohorte rétrospective auprès de 671 patients ambulatoires atteints d’une COVID-19 diagnostiquée à Toronto et confirmée en laboratoire entre le 1er mars et le 16 octobre 2020. Ils ont examiné l’association entre les caractéristiques de réfé- rence et les symptômes autodéclarés des patients au moment du diagnostic, d’une part, et le risque d’hospitalisation, d’admission en soins intensifs ou de décès par la suite, d’autre part.
Résultats : Des 671 participants, 26 (3,9 %) ont dû être hospitalisés, sept (1,0 %) ont été admis en soins intensifs et trois (0,4 %) sont décédés dans les 30 jours suivant le diagnostic. Les personnes de 65 ans ou plus étaient plus susceptibles de devoir être hospitalisées (RC 5,29, IC à 95 % 2,19 à 12,77) et celles qui n’avaient pas d’autres problèmes de santé l’étaient moins (RC 0,02, IC à 95 % 0,00 à 0,17). Après redressement pour tenir compte de l’âge et de la présence d’autres problèmes de santé,
la production de mucus (RC ajusté [RCa] 5,01, IC à 95 % 2,11 à 13,66), les arthralgies (RCa 4,82, IC à 95% 1,85 à 12,53), la diarrhée (RCa 4,56, IC à 95 % 1,82 à
11,42), la fièvre (RCa 3,64, IC à 95 % 1,50 à 8,82), les frissons (RCa 3,62, IC à 95 % 1,54 à 8,50) et la fatigue (RCa 2,59, IC à 95 % 1,04 à 6,47) étaient associés à
des hospitalisations.
Conclusions : L’évaluation précoce des symptômes des patients ambulatoires atteints de la COVID-19 peut contribuer à dépister les personnes vulnérables à une détérioration clinique. Lorsque ce facteur s’ajoute à l’âge et à l’histoire de problèmes de santé, la symptomatologie fournit plus d’information pronostique aux cliniciens qui prennent en charge les patients atteints de COVID-19 en milieu ambulatoire. D’autres v études s’imposent pour déterminer si un suivi plus intense et une intervention précoce auprès des personnes très vulnérables peuvent modifier la trajectoire clinique et le pronostic des patients ambulatoires atteints de la COVID-19.
MOTS-CLÉS
COVID-19, hospitalisation, patients ambulatoires, symptômes
INTRODUCTION
Since December 2019, coronavirus disease 2019 (COVID-19) has affected more than 100 million people worldwide [1], and it has had a crippling effect on healthcare systems and the global economy. A large-scale epidemiologic study from China, where the pandemic originated, has shown that approximately 81% of individuals with COVID-19 will have mild to moderate infection. An additional 14% will have severe infection, characterized by the presence of dyspnea, elevated respiratory rate, hypoxia, or more than 50% lung involvement, and 5% of patients will have critical illness [2].
Early in the pandemic response, as several countries witnessed COVID-19 overwhelm their healthcare systems, it became critical to determine which patients would be at risk of severe outcomes such as acute respiratory distress syndrome and death. Several factors associated with poor prognosis have been identified, including increased age, medical comorbidities, and certain laboratory parameters such as lymphopenia and elevated inflammatory markers [2-4]. There have also been efforts to determine whether symptoms at the time of presentation to healthcare can predict illness severity, with dyspnea and gastrointestinal symptoms identified as potential predictors of severe disease [5-8]. However, less is known about predictors of severe disease and risk of hospitalization among outpatients with mild infection, who make up the majority of those affected by COVID-19. Two studies from the United States report that older age and the presence of medical comorbidities are risk factors for hospitalization among outpatients with COVID-19, but neither assessed whether patient symptomatology is associated with disease severity [9,10]. As clinicians and researchers learn more about symptomatology among outpatients with COVID-19, there is growing interest in trying to determine whether symptoms can also predict clinical outcomes in this population [11-13]. Identifying outpatients at risk for hospitalization and adverse outcomes is critical to guide risk stratification and clinical management of patients initially presenting with mild symptoms.
In this study, we describe a cohort of individuals in Toronto, Ontario, Canada, diagnosed with COVID-19 and followed in the outpatient setting. We report on the clinical characteristics of these individuals, as well as a detailed account of their initial symptoms and subsequent clinical outcomes. The objective of the study was to identify symptoms and clinical features that are associated with poor clinical outcomes, including hospitalization, progression to severe disease requiring admission to the intensive care unit (ICU), and death.
METHODS
Study design, setting, and participants
This is a retrospective cohort study of all consecutive individuals diagnosed with COVID-19 and followed by the COVID-19 Expansion to Outpatients (COVIDEO) program at Sunnybrook Health Sciences Centre (SHSC), a tertiary care hospital in Toronto [14]. COVID-19 diagnosis was based on detection of severe acute respiratory syndrome coronavirus 2 (SARSCoV-2) RNA on either a mid-turbinate or nasopharyngeal swab by real-time polymerase chain reaction. The program was launched on March 1, 2020, and all outpatients diagnosed with COVID-19 at SHSC (by the emergency department [ED], occupational health and safety, the COVID-19 Assessment Centre, or another SHSC-affiliated site) were consecutively enrolled in the program to avoid selection bias. Healthcare workers (HCWs) employed by SHSC (regardless of where testing occurred) were also enrolled. The last day of enrolment was October 16, 2020.
Participants were contacted by an infectious diseases physician or nurse practitioner for assessment and counselling through the COVIDEO program. Clinical assessments were performed virtually, either via the Ontario Telemedicine Network platform or by telephone, and all participants were outpatients at the time of their first assessment. Details of thestructured clinical assessments and framework for follow-up have previously been published [14]. Data were extracted for the purpose of this analysis from the structured clinical assessment forms. For individuals requiring hospitalization, data on timing and duration of hospitalization, admission to the ICU, mechanical ventilation, and death were collected from the electronic medical record. For the purposes of this study, only symptoms at the time of initial COVIDEO assessment were used in the analysis.
Contributors: Conceptualization, A Zhabokritsky, N Daneman, N Andany; Methodology, N Daneman, N Andany; Validation, N Daneman, N Andany; Formal Analysis,
A Zhabokritsky; Investigation, A Zhabokritsky, S MacPhee, J Estrada-Codecido, A Santoro, AK Chan, PW-H Lam, A Simor, JA Leis, S Mubareka; Resources, N Daneman,
S Mubareka, N Andany; Data Curation, A Zhabokritsky, S MacPhee, J Estrada-Codecido, A Santoro; Writing – Original Draft, A Zhabokritsky; Writing – Review and Editing, N Daneman, S MacPhee, J Estrada-Codecido, A Santoro, AK Chan, PW-H Lam, A Simor, JA Leis, S Mubareka, N Andany; Supervision, N Daneman, N Andany; Project Administration, J Estrada- Codecido; Funding Acquisition, N Daneman.
Funding: This work was supported by funding from the Sunnybrook COVID-19 Research Initiative.
Conflicts of interest: The authors have nothing to disclose.
Ethics
The Research Ethics Board of SHSC approved the involvement of human participants; informed consent was not required for this data analysis, given its retrospective nature.
Outcome measures
The primary outcome of interest was hospital admission
to an acute care unit within 30 days of COVID-19 diagnosis (binary outcome). Secondary outcomes included [1] the proportion of outpatients diagnosed with COVID-19
who subsequently required ICU admission within 30 days
of diagnosis, [2] the proportion of outpatients diagnosed
with COVID-19 who subsequently required invasive mechanical ventilation (intubation] within 30 days of diagnosis, and [3] the proportion of outpatients diagnosed with COVID-19 who died within 30 days of diagnosis.
Sample size calculation and statistical methods
Given an overall risk of hospitalization of 19% among individuals with COVID-19 [2], 221 patients were required to detect a 15% increase in hospitalization risk associated with a particular symptom of interest (a = 0.05, power = 0.80, if prevalence of symptom is 20%).
Demographic and clinical characteristics were summarized with median and interquartile range (IQR) for continuous variables and frequency and percentages for categorical variables. The proportion of outpatients experiencing hospitalization, ICU admission, invasive mechanical ventilation, and death were reported as frequencies
and percentages.
Univariable and multivariable analyses were performed using χ2 tests and logistic regression to examine the association of demographic and clinical variables with hospitalization. A separate model (accounting for age as a continuous variable and presence or absence of comorbidities as a binary variable) was performed for each symptom in the logistic regression. Symptoms that were associated with hospitalization in the adjusted analysis were then combined into a single binary variable (defined by the presence of any or none of the associated symptoms). We examined the association between these combined symptoms and hospitalization using a logistic regression model, adjusting for comorbidities and age. Presence or absence of comorbidities was identified as a potential confounder between symptoms and hospitalization because individuals with underlying comorbidities may experience more symptoms than their counterparts according to their baseline clinical status and are more likely to be hospitalized regardless of symptom severity. Similarly, older age was identified as a confounder because older individuals may have different COVID-19 symptomatology than younger individuals and are overall more likely to be hospitalized. Sensitivity (SN), specificity (SP), negative predictive value (NPV), and positive predictive value (PPV) were calculated for each symptom individually as well as for the combined variable of symptoms associated with hospitalization in multivariable analysis.
RESULTS
Outpatients with COVID-19
Of 675 individuals diagnosed with COVID-19 as outpatients, 671 were enrolled in the COVIDEO program between
March 1, 2020, and October 16, 2020. The demographic and clinical characteristics of participants are summarized in Table 1.
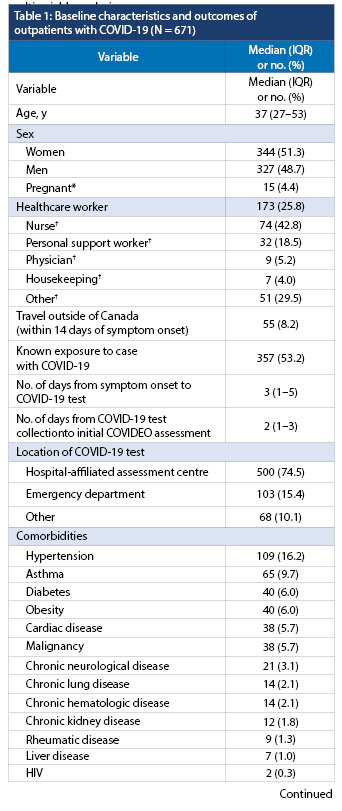
* Reported as percentage of women
† Reported as percentage of healthcare workers
‡ Reported as percentage of chest X-rays completed
IQR = Interquartile range; COVID-19 = Coronavirus disease
2019; COVIDEO = COVID-19 Expansion to Outpatients; ICU = Intensive care unit
The median (IQR) age of participants was 37 (27, 53) years, and half were women (51.3%). A quarter of participants were HCWs (25.8%). Half of individuals reported known exposure to a person with COVID-19 (53.2%), and few had travelled outside of Canada in the preceding 14 days (8.2%).
Most individuals were diagnosed with COVID-19 through the Assessment Centre (74.5%) or the ED (15.4%). The median (IQR) number of days from symptom onset to positive test was 3 [1,5], with a median 2 [1,3] days from specimen collection to initial assessment by the COVIDEO program. The most commonly reported comorbidities were hypertension (16.7%), lung disease (including asthma and other chronic lung diseases) (11.8%), diabetes (7.3%), and obesity (6.0%), but the majority of individuals had no baseline comorbidities (61.7%).
Clinical outcomes
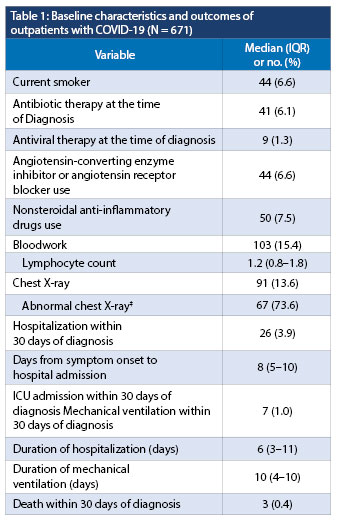
A total of 26 patients (3.9%) were hospitalized within 30 days of their diagnosis, with a median (IQR) of 8 [5,10] days from the time of diagnosis to hospitalization and a median duration of hospitalization of 6 [3,11] days. Seven of these individuals (1.0%, or 26.9% of those hospitalized) required admission to the ICU, and four of them were intubated (0.6%, or 15.4% of those hospitalized). There were three deaths in this cohort, resulting in a case fatality rate of 0.4%.
Clinical symptoms as predictors of clinical outcome and their diagnostic accuracy
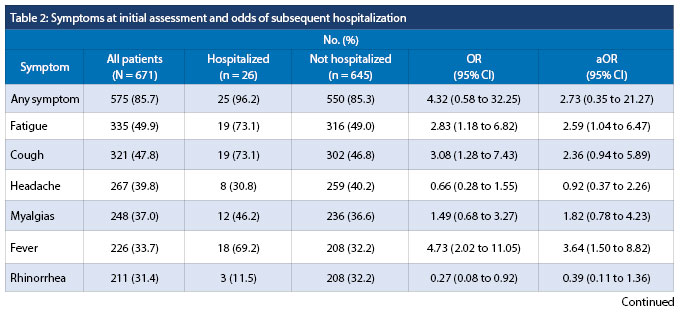
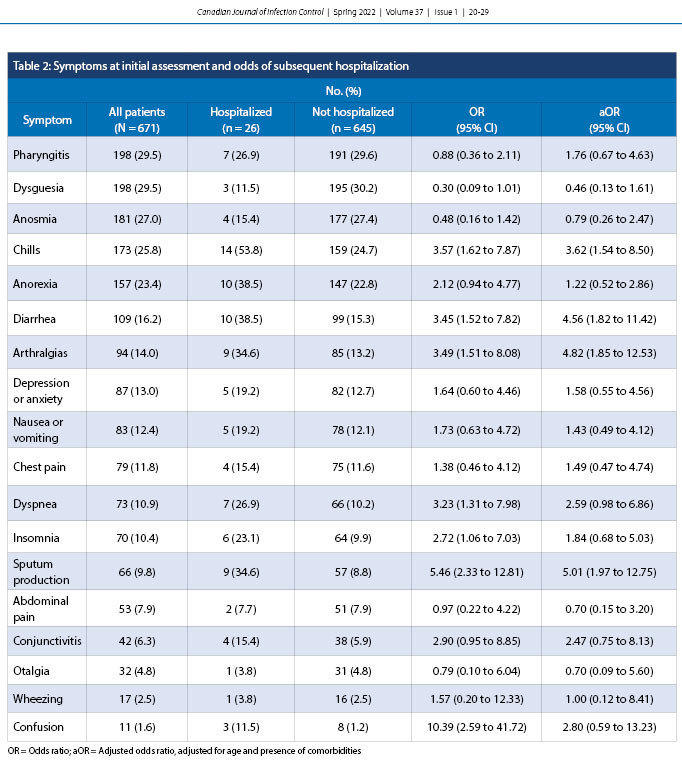
Symptoms reported by individuals at the time of their initial COVIDEO assessment are summarized in Table 2. A total of 96 individuals (14.3%) were asymptomatic. Fatigue (49.9%), cough (47.8%), headache (39.8%), myalgias (37.0%), and fever (33.7%) were the most commonly reported symptoms. After adjusting for age and presence of comorbidities, sputum production (adjusted odds ratio [aOR] = 5.01, 95% confidence interval [CI] 1.97 to 12.75), arthralgias (aOR = 4.82, 95% CI 1.85 to 12.53), diarrhea (aOR = 4.56, 95% CI 1.82 to 11.42), fever (aOR = 3.64, 95% CI 1.50 to 8.82), chills (aOR = 3.62, 95% CI 1.54 to 8.50), and fatigue (aOR = 2.59, 95% CI 1.04 to 6.47) were associated with subsequent hospitalization. Absence of these six symptoms was associated with significantly reduced odds of hospitalization, after adjusting for age and comorbidities (aOR = 0.09, 95% CI 0.01 to 0.69).
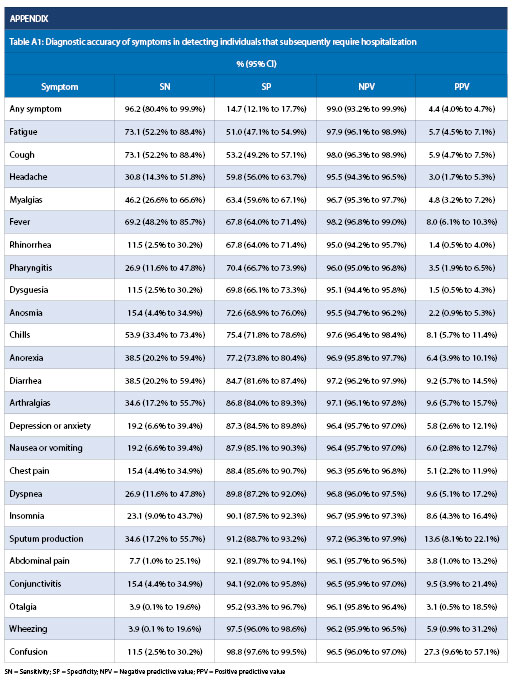
The proportion of initially asymptomatic individuals requiring hospitalization was lower relative to those with symptoms at the time of initial assessment (1.0% versus 4.3%, p = 0.120). The SN of individual symptoms ranged from 3.9% to 73.1%, and no individual symptom had sufficient SN to rule out subsequent hospitalization (Appendix Table A1). Absence of any symptom had an SN of 96.2% (95% CI 80.4% to 99.9%) and an NPV of 99.0% (95% CI 93.2% to 99.9%), which had similar diagnostic accuracy to the absence of the six symptoms associated with increased odds of hospitalization (SN of 96.2%, 95% CI 80.4% to 99.9%, and NPV of 99.6%, 95% CI 97.1%–99.9%).
Among all the reported symptoms, confusion (OR 10.90, 95% CI 1.20 to 99.08), chills (OR 7.38, 95% CI 1.42 to 38.40), and dyspnea (OR 6.36, 95% CI 1.40 to 9.02) were associated with increased odds of admission to the ICU. Confusion at the time of diagnosis was the only symptom associated with increased odds of death within 30 days of COVID-19 diagnosis (OR 32.90, 95% CI 2.75 to 393.01); however, this should be interpreted with caution because confusion affected only 11 individuals in the cohort with a resultant wide confidence interval.
Patient characteristics as predictors of clinical outcome
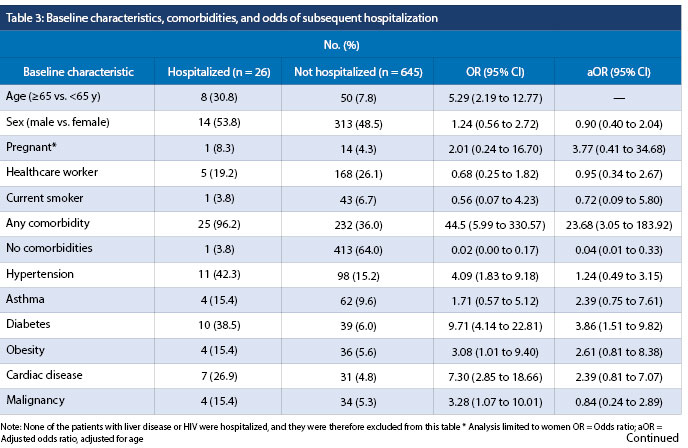
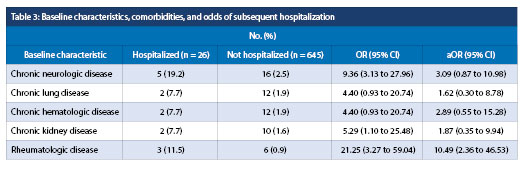
The median (IQR) age of the individuals who were hospitalized was 59.5 (53, 69.5) years, and it was 57 (49, 62) years among individuals who received ICU-level care and 83 (range 59-96) years among individuals who died within 30 days of their diagnosis. Overall, individuals aged 65 or older were more likely to require hospitalization (OR = 5.29, 95% CI 2.19 to 12.77) than younger individuals (Table 3). After adjusting for age, there was no significant difference in odds of hospitalization observed between women and men (aOR = 0.90, 95% CI 0.40 to 2.04). Comorbidities associated with hospitalization were rheumatologic disease (aOR = 10.49, 95% CI 2.36 to 46.53) and diabetes (aOR = 3.86, 95% CI 1.51 to 9.82). Presence of any comorbid condition was strongly associated with greater odds of hospitalization (aOR = 23.68, 95% CI 3.05 to 183.92), and having no history of comorbidities was associated with reduced odds of hospitalization (aOR = 0.04, 95% CI 0.01 to 0.33).
DISCUSSION
In this retrospective cohort study of outpatients with laboratory-confirmed COVID-19, individuals presenting with fever, chills, sputum production, diarrhea, fatigue, or arthralgias were more likely to require hospitalization during the course of their illness. In the absence of any of these symptoms, odds of hospitalization were significantly reduced with a high NPV. This suggests that symptomatology can facilitate risk stratification of outpatients with COVID-19 and help identify those who are at increased risk of poor clinical outcomes. Such individuals may warrant closer clinical monitoring, in-person assessment or benefit from early COVID-19-specific therapies. Conversely, targeted symptom assessment can provide clinicians with additional reassurance for low-risk patients and allow them to optimize resource allocation.
Symptoms associated with hospitalization in COVID-19 may provide insight into the pathogenesis of severe disease and motivators for seeking medical attention. For example, presence of fever, chills, and diarrhea can contribute to significant dehydration, especially among vulnerable elderly populations, but diarrhea has also been linked to the development of cytokine storm and multi-organ damage among people with COVID-19 [15,16]. Sputum production early in the disease process may be reflective of excessive mucus production, which contributes to hypoxia by altering the blood-gas barrier [17], and arthralgia may be an inflammatory manifestation of immune dysregulation [18,19].
Assessment of dyspnea remains an important challenge for clinicians. There have been several reports of silent hypoxemia among individuals with COVID-19 [20-22], and we recently demonstrated that presence or absence of dyspnea has limited accuracy for diagnosing hypoxemia [23]. Not surprisingly, although there was a trend toward greater odds of hospitalization among individuals reporting dyspnea, this was not statistically significant. Therefore, at-home pulse oximetry monitoring should be considered for individuals at high risk of clinical deterioration, even in the absence of dyspnea.
The presence of comorbid disease has been linked to increased risk of hospitalization and critical illness among people with COVID-19 [10,24,25]. In our cohort, patients requiring hospitalization were more likely to have diabetes and rheumatologic disease, regardless of age. Those with no comorbidities had significantly reduced odds of hospitalization. Similar to prior reports [3,24,26], older age was associated with greater odds of hospitalization. Smoking status was not associated with hospitalization, but there is ongoing controversy in the literature about the role of smoking as it relates to severity of COVID-19 infection [27-29]. In terms of other baseline characteristics, we did not find a difference in the odds of hospitalization between women and men, although several studies have reported greater risk of hospitalization [30] as well as admission to ICU and death among men [25,31,32].
LIMITATIONS
This study had a number of strengths related to the inclusion of all consecutive patients with COVID-19 and the design of the comprehensive symptom assessment at the time of diagnosis coupled with prospective monitoring of patients for clinical outcomes, reducing recall bias, and no loss to follow-up. However, it had several limitations. First, young individuals made up a large proportion of the study population, contributing to a low number of clinical outcome events. This limited our statistical power, resulted in wide confidence intervals, and prohibited looking at combinations of symptoms as predictors of clinical outcomes. Although we were able to adjust our analysis for age and presence of comorbidities, we did not account for other potential confounders influencing the association of symptoms and clinical outcomes to avoid model overfitting. Second, in this analysis we looked at symptoms around the time of diagnosis and did not account for symptoms that may develop during the course of illness and how they influence clinical outcomes. Although there was a median interval of 5 days between symptom onset and initial assessment, potentially contributing to recall bias, this is the time point when most patients come to medical attention, and thus the results are applicable to clinical practice. Finally, we assessed for hospitalization and death by reviewing clinical charts and a provincewide electronic system, which would have missed patients hospitalized outside the province or country or those who died at home without seeking medical attention, which we anticipate being an extremely uncommon occurrence (three-month follow-up for this cohort is ongoing to ensure outcomes were not missed).
CONCLUSIONS
Our study provides an overview of the clinical course of individuals with mild COVID-19 who were deemed appropriate for outpatient care at the time of diagnosis.
This population is representative of the majority of individuals with COVID-19 seen during the first 8 months of the pandemic in Canada and offers insight into symptoms and clinical characteristics associated with subsequent disease progression. We confirm that individuals aged 65 years or older and those with comorbidities (especially diabetes and rheumatologic disease) are at an elevated risk of progressing to more severe disease and should be prioritized in terms of clinical monitoring. In addition to this, presence of specific symptoms (including fever, chills, sputum production, diarrhea, fatigue, or arthralgias) can help identify individuals at risk of disease progression across ages and among those with or without comorbidities. Absence of these symptoms has a high NPV, providing clinicians with reassurance about the clinical trajectory.
Identifying individuals with mild COVID-19 who are at risk of hospitalization, critical illness, or death can help clinicians more efficiently triage patients and dedicate limited resources appropriately, such as providing close clinical follow-up or arranging for at-home pulse oximetry monitoring. Whether more intense follow-up or early intervention among high-risk individuals can alter the clinical trajectory and outcomes among outpatients with COVID-19 warrants additional study.
REFERENCES
1. World Health Organization. COVID-19 weekly epidemiological update. 2021. https://www.who.int/docs/default-source/coronaviruse/situation-reports/20210309_weekly_epi_update_30.pdf?sfvrsn=4e7da248_8&download=true (Accessed March 12, 2021)
2. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020;323(13):1239–42. https://doi.org/10.1001/jama.2020.2648.
3. Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective study. Lancet. 2020; 385(10229):1054. https://doi.org/10.1016/S0140-6736(20)30566-3.
4. Lighter J, Phillips M, Hochman S, et al. Obesity in patients younger than 60 years is a risk factor for COVID-19 hospital admission. Clin Infect Dis. 2020; 71(15):896–97. https://doi.org/10.1093/cid/ciaa415.
5. Ryan C, Minc A, Caceres J, et al. Predicting severe outcomes in Covid-19 related illness using only patient demographics, comorbidities and symptoms. Am J Emerg Med. 2020;45:378–84. https://doi.org/j.ajem.202.09.017.
6. Adnan D, Deshmukh AA, Khan SR, et al. Gastrointestinal symptoms predict the outcomes of COVID-19 infection. Am J Gastro. 2020;115:S685–S686. https://doi. org/10.14309/01.ajg.0000707480.23480.66.
7. Abayomi A, Odukoya O, Osibogun A, et al. Presenting symptoms and predictors of poor outcomes among 2,184 patients with COVID-19 in Lagos State, Nigeria. Int J Infect Dis. 2021;102:226–32. https://doi.org/10.1016/j.ijid.2020.10.024.
8. Jehi L, Ji X, Milinovich A, et al. Development and validation of a model for individualized prediction of hospitalization risk in 4,536 patients with COVID-19. PLoS One. 2020;15(8):e0237419. https://doi.org/10.1371/journal.pone.0237419.
9. Garg S, Kim L, Whitaker M, et al. Hospitalization rates and characteristics of patients hospitalized with laboratory-confirmed coronavirus disease 2019—COVID-NET, 14 states, March 1-30, 2020. Morb Mortal Wkly Rep. 2020;69(15):45. https://doi.org/10.15585/mmwr.mm6915e3.
10. Petrilli CM, Jones SA, Yang J, et al. Factors associated with hospital admission and critical illness among 5,279 people with coronavirus disease 2019 in New York City: a prospective cohort study. BMJ. 2020;369:m1966. https://doi.org/10.1136/bmj.m1966.
11. Blair PW, Brown DM, Jang M, et al. The clinical course of COVID-19 in the outpatient setting: a prospective cohort study. OFID. 2021;8(2):ofab007. https://doi.org/10.1101/2020.09.01.20184937.
12. Sudre CH, Lee KA, Lochlainn MN, et al. Symptom clusters in COVID-19: a potential clinical prediction tool from the COVID Symptom Study app. Sci Adv. 2021;7(12):eabd4177. https://doi.org/10.1126/sciadv.abd4177.
13. Vahey GM, Marshall KE, McDonald E, et al. Symptom profiles and progression in hospitalized and nonhospitalized patients with coronavirus disease, Colorado, USA, 2020. Emerg Infect Dis. 2021;27(2):385–95. https://doi.org/10.3201/eid2702.203729.
14. Lam PW, Seghal P, Andany N, et al. A virtual care program for outpatients diagnosed with COVID-19: a feasibility study. CMAJ Open. 2020;8(2): E407. https://doi.org/10.9778/cmajo.20200069.
15. Zhang L, Han C, Zhang S, et al. Diarrhea and altered inflammatory cytokine pattern in severe coronavirus disease 2019: impact on disease course and in-hospital mortality. J Gastroenterol Hepatol. 2021;36(2):421–29. https://doi.org/10.1111/jgh.15166.
16. Wan Y, Li J, Shen L, et al. Enteric involvement in hospitalized patients with COVID-19 outside Wuhan. Lancet Gastroenterol Hepatol. 2020;5(6):534–5. https://doi.org/10.1016/S2468-1253(20)30118-7.
17. Liu Y, Lv J, Liu J, et al. Mucus production stimulated by IFN-AhR signaling triggers hypoxia of COVID-19. Cell Res. 2020;30:1078–87. https://doi.org/10.1038s41422-020-00435-z.
18. Hoong CWS, Amin MNME, Tan TC, Lee JE. Viral arthralgia a new manifestation of COVID-19 infection? A cohort study of COVID-19-associated musculoskeletal symptoms. Int J Infect Dis. 2021;18(104):363–9. https://doi.org/10.1016/j.ijid.2021.01.031.
19. Parisi S, Borrelli R, Bianchi S, Fusaro E. Viral arthritis and COVID-19. Lancet Rheumatol. 2020;2(11):e655–7. https://doi.org/10.1016/S2665-9913(20)30348-9.
20. Chandra A, Chakraborty U, Pal J, Karmakar P. Silent hypoxia: a frequently overlooked clinical entity in patients with COVID-19. BMJ CP. 2020;13:e237207. https://doi.org/10.1136/bcr-2020-237207.
21. Wilkerson RG, Adler JD, Shah NG, Brown R. Silent hypoxia: a harbinger of clinical deterioration in patients with COVID-19. Am J Emerg Med. 2020;38(10):2243.e5–2243.e6. https://doi.org/10.1016/j.ajem.2020.05.044.
22. Brouqui P, Amrane S, Million M, et al. Asymptomatic hypoxia in COVID-19 is associated with poor outcome.
Int J Infect Dis. 2021;102:233–8. https://doi.org/10.1016/j.ijid.2020.10.067.
23. Berezin L, Zhabokritsky A, Andany N, et al. Diagnostic accuracy of subjective dyspnoea in detecting hypoxaemia among outpatients with COVID-19: a retrospective cohort study. BMJ Open. 2021;11:e046282. https://doi.org/10.1136/bmjopen-2020-046282.
24. Tenforde MW, Billig Rose E, Lindsell CJ, et al. Characteristics of adult outpatients and inpatients with COVID-19—11 academic medical centers, United States, March-May 2020. Morb Mortal Wkly Rep. 2020;69(26):841–6. https://doi.org/10.15585/mmwr.mm6926e3.
25. Jain V, Yuan JM. Predictive symptoms and comorbidities for severe COVID-19 and intensive care unit admission: a systematic review and meta-analysis. Int J Public Health. 2020;65(5):533–46. https://doi.org/10.1007/s00038-020-01390-7.
26. CDC COVID-19 Response Team. Severe outcomes among patients with coronavirus disease 2019 (COVID-19)—United States, February 12–March 16, 2020. Morb Mortal Wkly Rep. 2020;69:343–6. https://doi.org/10.15585/mmwr.mm6912e2.
27. Guo FR. Active smoking is associated with severity of coronavirus disease 2019 (COVID-19): an update of a metaanalysis. Tob Induc Dis. 2020;18:37. https://doi.org/10.18332/tid/121915.
28. Lippi G, Henry BM. Active smoking is not associated with severity of coronavirus disease 2019 (COVID-19). Eur J Intern Med. 2020;75:107–8. https://doi.org/10.1016/j.ejim.2020.03.014.
29. Vardavas CI, Nikitara K. COVID-19 and smoking: a systematic review of the evidence. Tob Induc Dis. 2020;18:20. https://doi.org/10.18332/tid/119324.
30. Jin JM, Bai P, He W, et al. Gender differences in patients with COVID-19: focus on severity and mortality.
Front Public Health. 2020;8:152. https://doi.org/10.3389/fpubh.2020.00152.
31. Intensive Care National Audit & Research Centre. ICNARC report on COVID-19 in critical care. 2020. https://www.icnarc.org/DataServices/Attachments/Download/da19fd54-70b2-ea11-9127-00505601089b (Accessed March 12, 2021)
32. Remuzzi A, Remuzzi G. COVID-19 and Italy: what next? Lancet. 2020;395:1225–1228. https://doi.org/10.1016/S0140-6736(20)30627-9.